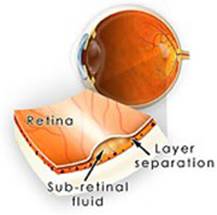
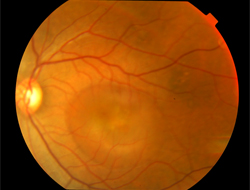
CSR occurs when a small break
forms in the outer pigmented layer of the
retina. Clear fluid from the layer of blood
vessels that lie
underneath the retina seeps
up through the break, causing a small
detachment to form under the retina.
This
problem is somewhat similar to a water
blister that forms on the skin. The process
is similar to CSR: fluid collects beneath
the skin's surface, causing the layers of
skin to separate.
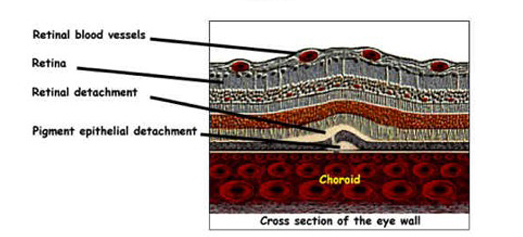
The retinal pigment
epithelium is a single-celled layer that
lies between the retina and the choroids.
This tissue layer normally serves to prevent
fluid from the choroidal circulation from
leaking under the retina. In central serous,
fluid equilibrium is disturbed leading to
leakage beneath the retina which elevates it
to produce a macular detachment which
distorts vision.
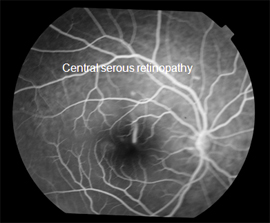
Central serous retinopathy is a slight
accumulation of fluid in the macular (center
of the retina) region of the eye that lies
between the retinal pigment epithelium (the
pigmented cell layer just outside the
neurosensory retina that nourishes retinal
visual cells) and the outer segments. A
relative central scotoma (area of lost or
depressed vision within the visual field
surrounded by an area of less depressed or
normal vision) results, but usually resolves
spontaneously within a few months. Serous
means thin and watery-like serum. Central
serous retinopathy is characterized by an
accumulation of transparent fluid at the
posterior pole of the fundus (base), causing
a circumscribed area of retinal detachment
at the posterior pole. When left alone,
central serous retinopathy heals
spontaneously within 6 months (average 3-4
months), with full recovery of visual
acuity. However, about one-third to one-half
of all patients have recurrences after the
first episode of the disease; 10 percent
have three or more recurrences. In almost
half of the patients, the recurrence is
within one year of the primary episode, but
relapses may occur up to ten years later.
Causes and Risk Factors: The disease
primarily affects young adults ages 20 to
45. Men are affected ten times frequently
than women. CSR is sometimes calledidiopathicCSRwhich
means that its cause is unknown.
Nevertheless, stress appears to play an
important role. An oft-cited but potentially
inaccurate conclusion is that persons in
stressful occupations, such as airplane
pilots, have a higher incidence of CSR. The
"type A personality" has also been linked to
this condition. However, the statistics may
be skewed by the fact that CSR often goes
undiagnosed or misdiagnosed; airline pilots
and so-called "type A" people are
demonstrably exacting, demanding people with
(certainly in the case of pilots)
better-than-average vision. They are more
likely than the general population to notice
the sometimes-subtle degradation of vision
caused by CSR and insist on a believable
diagnosis of it. People who need glasses may
assume that the blurriness caused by CSR is
simply a change in their prescription, and
fail to have the condition assessed by a
retinal specialist. These statistic-skewing
factors undermine the conclusion that CSR is
a condition specific to "type A" people.
CSR has also been associated with cortisol
and corticosteroids, and persons with higher
levels of cortisol than normal also have a
higher propensity to suffer from CSR.
Cortisol is a hormone secreted by the
adrenal cortex which allows the body to deal
with stress, which may explain the
CSR-stress association. There is extensive
evidence to the effect that corticosteroids
("cortisone") --- commonly used to treat
inflamations, allergies, skin conditions and
even certain eye conditions --- can trigger
CSR, aggravate it and cause relapses.
The incidence of CSR in persons with
Cushing's syndrome 5%. Cushing's syndrome is
characterized by very high cortisol levels.
SIGNS AND SYMPTOMS
Many patients first notice a
minor blurring of vision, followed by
various degrees of:
metamorphopsia (defective, distorted vision)
micropsia (distorted visual perception in
which objects appear smaller than their
actual size)
chromatopsia (visual defect in which objects
appear unnaturally colored)
central scotoma
increasing hyperopia (farsightedness)
Visual acuity in the acute
stage may range from 20/20 to 20/200 and
averages 20/30. In some patients the onset
of symptoms is preceded or accompanied by
migraine-like headaches.
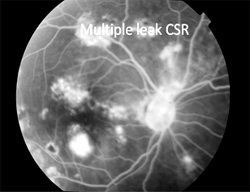
DIAGNOSIS:
The diagnosis usually starts
with a dilated examination of the retina,
followed with confirmation byOCTand
orfluorescein
angiography. The angiography test will
usually show one or more fluorescent spots
with fluid leakage. In 10%-15% of the cases
these will appear in a "classic" smoke stack
shape. AnAmsler
gridmay
be useful in documenting the precise area of
the visual field involved.
Prognosis:Most
patients with central serous retinopathy
will spontaneously recover visual acuity in
six months (average time to recovery three
to four months). Many patients will have
some residual symptoms, such as distortion,
decreased color and contrast sensitivity,
and visual difficulty at night. Despite an
overall good prognosis, 40 to 50 percent of
patients experience at least one recurrence.
TREATMENT:
Although no medication has
thus far proved effective in treating
central serous retinopathy, a beneficial
effect of laser photocoagulation has been
reported in several studies. Findings
indicate that direct photocoagulation of the
leakage point not only shortens the acute
phase of the disease but also lowers the
recurrence rate to about one fifth of what
would be expected without active treatment.
If possible, any ongoing corticosteroid
treatment including nasal sprays, skin
creams, inhalers and oral medications should
be stopped.