Another type of surgery that can be done for
some retinal detachments is called pneumatic
retinopexy. Pneumatic retinopexy is
performed in the office using local
anesthesia.
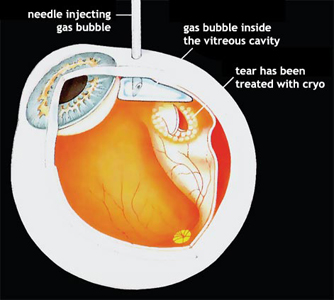
Cryotherapy or laser treatment is performed
to seal the retinal tear. Instead of placing
a scleral buckle on the outside of the eye,
using a needle, the surgeon injects a gas
bubble inside the vitreous cavity of the
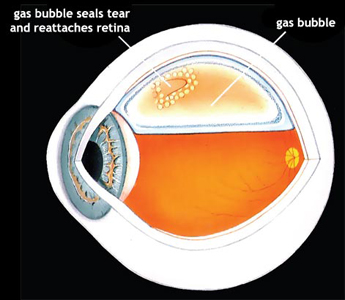
eye. The patient is instructed to keep his
or her head in a specific position so that
the gas bubble pushes the detached retina
against the back wall of the eye to seal the
retinal tear. The patient is asked to remain
in this position for a period of time until
the retinal tear is sealed against the back
wall of the eye. Your surgeon will tell you
how long special positioning is necessary.
The gas bubble in the vitreous cavity of the
eye expands for several days and takes two
to six weeks to disappear. During this time,
airplane travel or travel to a high altitude
must be avoided because high altitudes can
result in an expansion of gas and an
increase in pressure that can damage the
eye. Your surgeon will tell you when it is
safe to travel.
It is also important for a patient with a
gas bubble not to lie face up, as the gas
bubble will come to rest against the lens of
the eye and may cause a cataract or high
pressure in the eye. Antibiotic eye drops
may be used during the days following the
surgery.
The chance of successfully reattaching the
retina with pneumatic retinopexy is slightly
less than with a vitrectomy or scleral
buckle . But with pneumatic retinopexy,
hospitalization, general anesthesia, and the
cutting that is necessary with scleral
buckling surgery are all avoided. Pneumatic
retinopexy cannot be used for every retinal
detachment. Your surgeon will discuss with
you whether pneumatic retinopexy is feasible
and the chances for successfully reattaching
your retina. Complications of pneumatic
retinopexy include cataract formation,
glaucoma, gas getting under the retina,
excessive scar tissue formation, and
infection. Any one of these complications
can lead to a total loss of vision, but each
is rare. The most common complication is the
formation of new retinal tears and
recurrence of the retinal detachment. If the
retina becomes detached again, scleral
buckling surgery or vitrectomy can usually
be performed to reattach it.